Virtual Asynchronous Ward for Rapid Up-Titration in Heart Failure
Summary
- All patients were rapidly up-titrated to the maximum tolerated dose over 4 weeks
- Zero heart failure readmission after 30 days
- All patients on the virtual ward felt safe and were 100% satisfied
- Resource efficient and safe

The Problems
The publication of the STRONG-HF trial highlights the importance of prompt up-titration of the four pillar heart failure medications.
However, existing hospital pathways would find these challenging given constraints on staffing and appointment availability. As a result, patients may not receive the benefits of these drugs, which include fewer hospitalisations and reduced mortality.
A potential solution could be remote monitoring in a virtual ward to enable prompt up-titration of the four pillars via an asynchronous clinic.
The Goals
- Rapidly up-titrate patients to the 4 pillars of medication in 4 weeks
- Enable clinicians to easily make appropriate patient assessment to safely achieve maximum tolerated dose
- Improve patient outcomes
The Ortus Solution
Barts Heart Centre has been using the Ortus-iHealth remote patient monitoring platform to deliver the virtual asynchronous ward.
- 27 newly diagnosed heart failure patients were onboarded onto the virtual ward between April 2023 and August 2023. They were registered on to the Ortus-iHealth remote monitoring platform following an initial face to face or remote telephone.
- All 27 patients had an initial ejection fraction <40% with a mean age of 62.
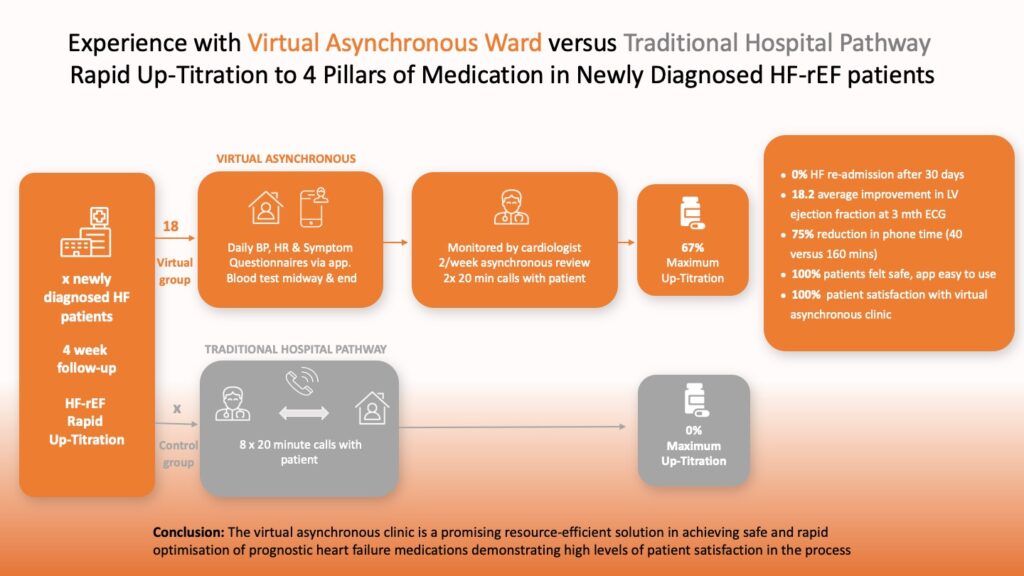
- Patients submitted daily readings of their blood pressure, heart rate and any symptoms via the Ortus-iHealth patient app.
- Clinicians used the Ortus-iHealth remote patient monitoring platform and dashboard to review the patient and their data in eight asynchronous appointments (2 per week) where medication changes would be suggested.
- Two blood tests at the midpoint and the end were arranged to monitor renal function.
- Patient feedback was obtained via a standard questionnaire.
- Data was also collected from a control group who received up-titration via existing pathways.
Ortus-iHealth provides clinicians with a digital platform to remotely monitor patients, communicate, schedule appointments, manage consent and deliver patient education and information. Patients use the Ortus-iHealth app on their smartphones to respond to questionnaires and submit vital signs which are monitored by clinicians.
Data received daily from patient questionnaires and remote monitoring of patient vital signs is evaluated by clinicians through the Ortus-iHealth dashboard. This enables clinicians to accurately determine the progression of a patient’s condition and the appropriateness of ongoing medication up-titration.
Rapid Medication Up-Titration in Newly Diagnosed Heart Failure
Results

The virtual asynchronous clinic is a promising resource-efficient solution in achieving safe and rapid optimisation of prognostic heart failure medications demonstrating high levels of patient satisfaction in the process
- All patients were rapidly up-titrated to the maximum tolerated dose over 4 weeks
- Zero heart failure readmission after 30 days
- All patients on the virtual ward felt safe and were 100% satisfied
- Resource efficient and safe